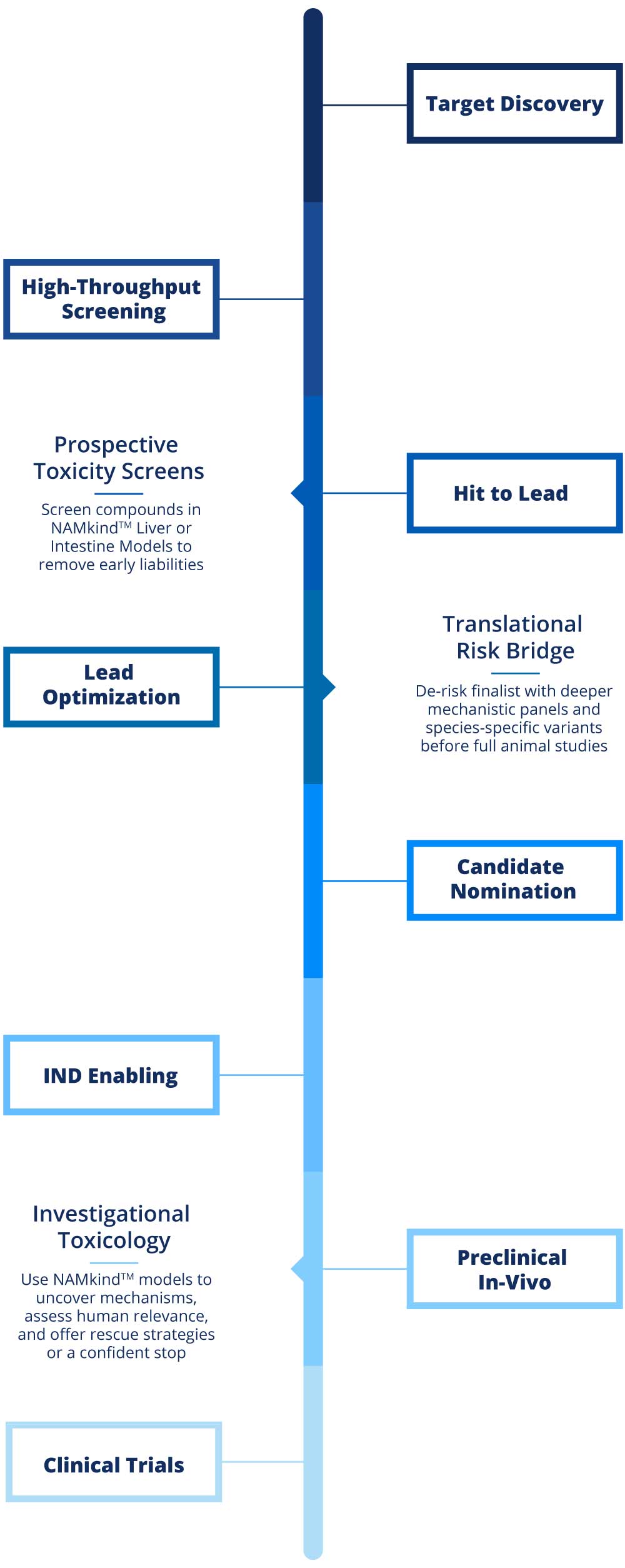
VivoSim Labs anchors its NAMkind™ services at three decision-critical points.
Prospective Screens during Hit-to-Lead and early Lead Optimization. In two weeks, our Liver and Intestine models can screen 20+ compounds, flag early liabilities through core biomarkers, and deliver insights that guides chemistry toward safer compounds
Translational Bridge begins in late Lead Optimization and continues through Candidate Nomination. Here we deploy species-specific models plus optional mechanistic panels to confirm human relevance, fine-tune safety margins, and supply regulatory-ready narratives before and throughout IND-enabling studies
Investigative Toxicology is an on-demand service activated when unexpected findings emerge in animal or human studies. The same NAMkind™ models reproduce or refute the signal, map root-cause pathways and provide clear go, modify or stop recommendations within weeks
Target Discovery
Hit to Lead
Translational
Risk Bridge
De-risk finalist with deeper mechanistic panels and species-specific variants before full animal studies
Candidate Nomination
Preclinical In-Vivo
High Throughput Screening
Prospective
Toxicity Screens
Screen compounds in NAMkindTM Liver or Intestine Models to remove early liabilities
Lead Optimization
IND Enabling
Investigational
Toxicology
Use NAMkindTM models to uncover mechanisms, assess human relevance, and offer rescue strategies or a confident stop
Clinical Trials
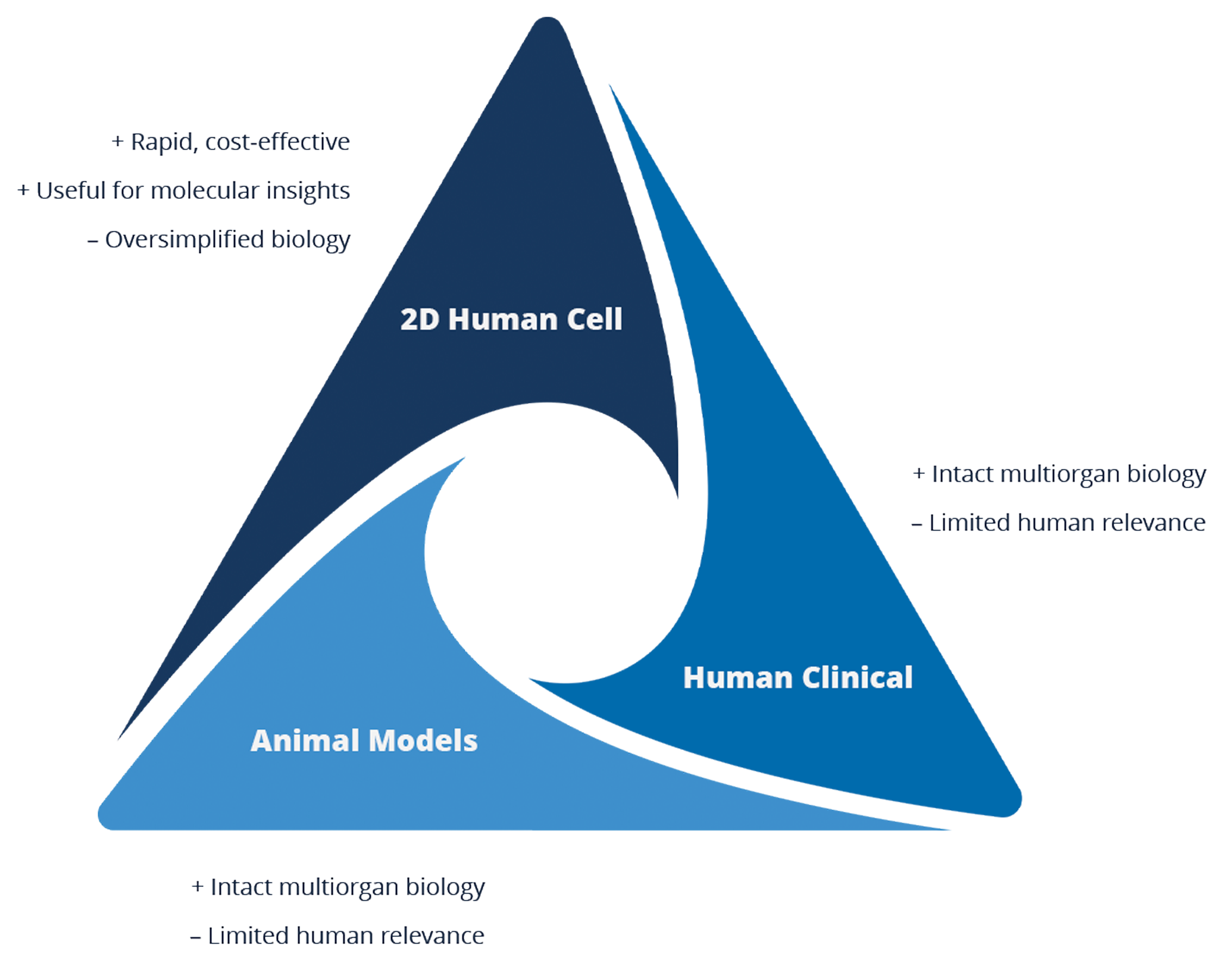
What is NAM/NAMkind
To overcome the limitations of traditional toxicity testing, New Approach Methodologies (NAMs) aim to be more informative, faster, more cost-effective. The goal is to reduce or replace animal testing using validated and reliable 3D and tissue-based models.
VivoSim’s NAMkind™ models utilize primary human cells to create micro-liver and micro-intestine organoids that more accurately reflect relevant biological responses than traditional toxicology tests. The NAMkind™ Liver and NAMkind™ Intestine models are specifically designed to help customers identify and overcome toxicology challenges, driving drug advancement in a timely and safe manner.